Open Letter to Secretary Doug Collins, U.S. Department of Veterans Affairs
Exposing the VA's Fraudulent SOP: A Call for Accountability on TERA, the Toxicity of COVID-19 Injections, Unlawful Mandates, and the Betrayal of Service Members
Open Letter to Secretary Doug Collins, U.S. Department of Veterans Affairs
March, 2025.
The Honorable Doug Collins Secretary of Veterans Affairs Department of Veterans Affairs
Subject: Immediate Action Required: Correcting VA Policy on ‘Vaccine’ Injuries and Addressing Exclusion from Toxic Exposure Risk Activity (TERA)
Dear Secretary Collins, Congratulations on your appointment as Secretary of Veterans Affairs. Your leadership comes at a crucial time for the Department, which is currently faced with a critical legal and scientific issue— the persistent denial of vaccine and vaccine-like gene therapy technologies-induced injuries as a form of toxic exposure risk for military personnel and veterans. The current VA Standard Operating Procedure (SOP) excludes vaccines as a TERA-related injury. This issue is particularly concerning given the lack of comprehensive recognition within current policy frameworks, including the Toxic Exposure Risk Activity (TERA) provisions, despite emerging scientific evidence that links such injuries to long term adverse health effects.
Here is the current VA SOP:
“Vaccines and medications in general are not considered participation in a Toxic Exposure Risk Activity (TERA) because there is no scientific or medical evidence that supports the conclusion that vaccines and medications administered to Service Members have resulted in long-term adverse health effects.”
The contradiction in the SOP is that the VA acknowledges toxic exposure under TERA for military occupational hazards, asbestos, and other service-related exposures—even when long-term health effects are uncertain—but then arbitrarily excludes vaccines and medications. If TERA is supposed to cover all potential toxic exposures from military service, then there’s no valid reason to preemptively exempt vaccines. Without this note, vaccine-related injuries would have to be evaluated under TERA like any other exposure. This policy isn’t based on evidence; it’s a deliberate carve-out to prevent claims.
The VA cannot claim to follow a scientific standard while applying different rules to different exposures based on policy convenience.
Further, the mandated exposure of military personnel to potentially harmful substances, including COVID-19 injections, poses a direct and significant risk to the health and operational readiness of our armed forces. This issue is particularly concerning as it violates the core principles of informed consent and individual autonomy, undermining the health and well-being of both our active service members and veterans.
As Secretary of Veterans Affairs, it is your critical responsibility to ensure that the VA acknowledges and addresses the long-term risks associated with these mandates. Failing to recognize the potential harm of vaccine-induced injuries compromises not only the readiness of our military forces but also the integrity of the care provided to those who have served.
The toxicity associated with these injections is undeniable. Substances like N1 Methyl-Pseudouridine (N1-MPU) and polyethylene glycol (PEG)-lipids, both engineered for enhanced durability and activity in biological systems, present long term risks to those exposed. N1-MPU, a modified nucleoside in mRNA vaccines, is specifically designed to evade immune recognition, but its synthetic nature raises significant concerns regarding mutagenic potential, which could increase the risk of adverse genetic effects (Kowarz et al., 2021). PEG-lipids, added to mRNA vaccines to stabilize lipid nanoparticles (LNPs) that deliver the mRNA into cells, are known to induce severe immune reactions, leading to conditions such as anaphylaxis (Szebeni et al., 2018). These synthetic components bypass natural metabolic defenses and can cause harm that may not become fully evident until years later. This type of engineered exposure cannot be ignored, and it is unacceptable to treat these substances as innocuous when the evidence overwhelmingly points to their profound impact on the health of our veterans.
The evidence for categorizing these substances under the Toxic Exposure Risk Activity (TERA) is substantial. N1-Methyl-Pseudouridine (N1-MPU), integrated into mRNA vaccines, not only evades immune surveillance but also hints at potential genetic instability due to its synthetic nature (Kowarz et al., 2021).
This raises concerns about its potential to alter genetic material over time, a risk not adequately addressed under current VA policies. Polyethylene glycol (PEG)-lipids, essential for stabilizing lipid nanoparticles (LNPs) in mRNA vaccines, have been documented to trigger severe immunological reactions, including anaphylaxis. Studies have shown that PEG can lead to the production of anti-PEG antibodies, which can result in acute hypersensitivity reactions (Szebeni et al., 2018). Furthermore, LNPs themselves contribute to systemic toxicity through mechanisms like inflammation and damage to endothelial cells, potentially leading to cardiovascular issues such as myocarditis (Bahl et al., 2017). Biological Agents and Legal Prohibitions: Beyond chemical toxicity, there's the issue of biological agents.
The mRNA vaccines encode for the spike protein of SARS-CoV-2, which, once expressed, can lead to prolonged presence in the body, contributing to chronic inflammation, autoimmune responses, and vascular issues, including thrombosis (Kowarz et al., 2021). The spike protein's interaction with human cells has been associated with both acute and long-term health effects, which underscores the need for these vaccines to be considered under TERA. Legally, the use of biological agents, particularly in a mandatory context, is highly scrutinized.
The National Defense Authorization Act (NDAA) includes provisions that prohibit the Secretary of Defense (SECDEF) from mandating the use of biological agents on troops without explicit consent under certain conditions. Specifically, Section 705 of the NDAA for Fiscal Year 2006 (10 U.S.C. § 1107) restricts the use of "investigational new drugs" or biological agents in military settings unless they meet specific criteria, including informed consent, unless waived under very specific emergency scenarios. The application of mRNA vaccines, which encode foreign proteins, could be considered within this legal framework due to their biological activity and potential for long-term health impacts.
Given these scientific and legal aspects, it's critical to reassess how these substances and their biological outcomes are handled under TERA. The synthetic components and biological effects of mRNA vaccines necessitate a thorough review to align with the VA's duty to protect and compensate veterans exposed to toxic substances during their service.
Restated: The current VA policy stance—refusing to classify mandated COVID 19 injections under Toxic Exposure Risk Activity (TERA) standards—is not only scientifically indefensible but also a direct betrayal of the trust and well-being of our nation’s veterans. The implementation of a fraudulent Standard Operating Procedure (SOP) explicitly prohibiting claims processors from applying toxic exposure criteria to vaccine injuries has effectively blocked countless veterans from receiving the care and compensation they deserve. Scientific Evidence of Toxic Exposure: The body of research surrounding the toxicity of vaccine components has grown significantly. Studies show: • Lipid Nanoparticles (LNPs): These nanoparticles, used to deliver mRNA into cells, have been linked to inflammation and damage to endothelial cells, contributing to cardiovascular issues like myocarditis. Accumulation of LNPs in vital organs has been documented in both preclinical and clinical studies, leading to concerns about long-term toxic effects, particularly in vulnerable populations like veterans exposed to multiple toxins during service (Bahl et al., 2017). • Spike Proteins: The persistent presence of spike proteins in the body, especially those produced by mRNA vaccines, has been associated with chronic inflammation, autoimmune disorders, and vascular damage, such as blood clotting and myocarditis. Spike proteins have been found to remain in the bloodstream and tissues for months, far beyond the expected timeline of vaccine efficacy (Kowarz et al., 2021). • DNA Contamination in mRNA Injections: Recent studies have raised concerns about DNA contamination in mRNA vaccine formulations, which could lead to mutagenic effects. This contamination may pose significant risks, particularly given the military’s frequent exposure to other toxic substances (e.g., burn pits, PFAS, heavy metals), compounding the vulnerability of service members and veterans to further genetic damage (Wang et al., 2022).
These substances, along with others such as polyethylene glycol (PEG) and synthetic mRNA, qualify as toxic agents due to their potential for long-term harm. PEG, in particular, has been associated with allergic reactions and other severe immune responses in a subset of recipients, further demonstrating the risk associated with mandated inoculations. In addition to the known vaccine components, emerging evidence from research on lipid nanoparticles (LNPs) and PEG-lipids in gene therapies and vaccines reveals serious concerns. Studies have demonstrated that these lipid nanoparticles are prone to accumulating in various organs and tissues, leading to inflammatory responses and, in some cases, autoimmune diseases. For instance, a study published in Nature Biomedical Engineering shows that lipid nanoparticles used in mRNA vaccines can cause endothelial cell dysfunction, contributing to vascular damage and clot formation (Sahay et al., 2020). Additionally, PEG (polyethylene glycol), a component used in these lipid formulations, has been associated with hypersensitivity reactions, including anaphylaxis, and immune system activation (Allen et al., 2021).
These findings underscore the potential risks posed by these novel vaccine components, particularly in individuals with pre-existing vulnerabilities, such as our veterans. Furthermore, research in the journal Vaccine highlights the prolonged inflammatory responses triggered by these nanoparticles, which may exacerbate underlying conditions or even lead to new disorders, including neurological and cardiovascular conditions (Yoo et al., 2022). These findings suggest that the long term safety profile of these vaccines remains an open question, with serious implications for our troops who were subjected to these novel biologics under emergency conditions.
Additionally, veterans who were exposed to these substances during service have compromised detoxification pathways, making them more vulnerable to the additional risk posed by vaccine-induced injuries. This compounded exposure scenario aligns with established toxicity assessment principles, which indicate the need for a more comprehensive review and reconsideration of the VA’s stance on vaccine-induced injuries.
Urgent Actions Required: I respectfully urge you to take immediate action to:
1. Revisit and reverse the fraudulent SOP that blocks the classification of vaccine-induced injuries as part of Toxic Exposure Risk Activity (TERA).
2. Apply the same toxic exposure criteria to all mandated substances, including mRNA injections and their synthetic components.
3. Provide clear and transparent guidance to claims processors ensuring that veterans suffering from vaccine-related injuries receive the care and compensation they are entitled to.
Until this issue is addressed, veterans will continue to face unnecessary barriers to the care they need, while the long-term health consequences of these mandates remain unaddressed. Immediate and decisive action is required to restore integrity to the VA’s handling of toxic exposure claims and ensure that those who serve our country are not abandoned when they need help most.
As a leading advocate for service members and veterans affected by vaccine injuries, I respectfully request the opportunity to engage in a direct dialogue regarding critical concerns surrounding current VA policies and procedures, with a particular focus on the fraudulent Standard Operating Procedures (SOPs) and violations of established regulatory frameworks. These systemic issues have caused significant harm to the health and well-being of those who have served and sacrificed for our nation.
Given the urgency and severity of these matters, I am prepared to provide additional evidence, expert testimony, and firsthand accounts that will shed light on the harm caused by these policies. I believe that this information will be vital in addressing the longstanding injustices that have been unrecognized and unaddressed for far too long.
It is imperative that we take meaningful action to correct these failures. I am fully committed to ensuring that our troops and veterans receive the care and respect they rightfully deserve, and I would greatly appreciate the opportunity to present this crucial information in person. I look forward to your swift response and to working together toward a future where lasting change and accountability are realized.
On behalf of those who have been affected, I appreciate your time and your ongoing commitment to supporting those who have served.
Sincerely,
Dr. Crisanna Shackelford
Veteran. Leading Expert and Advocate for Vaccine Safety, DOD Vaccine Policy Reform, and TERA-Related Injuries Among Active-Duty Service Members and Veterans. Testimony and Advocacy at the Intersection of Military Health and Medical Freedom.
Follow me on X: @DrC_Shackelford Stay updated on advocacy efforts and support for those harmed by injections/vaccines through our nonprofit: @RealReactionsNP and here Real Reactions
Note: This article would not be possible without the countless individuals who have contributed their voices and knowledge, along with the brave whistleblowers who’ve come forward to reveal the full extent of this toxic injustice. Their collective efforts, along with the references and evidence shared throughout, highlight the urgency of addressing this issue and demanding the accountability our service members and veterans deserve. To Mr. Sonny Fleeman - Thank you!!
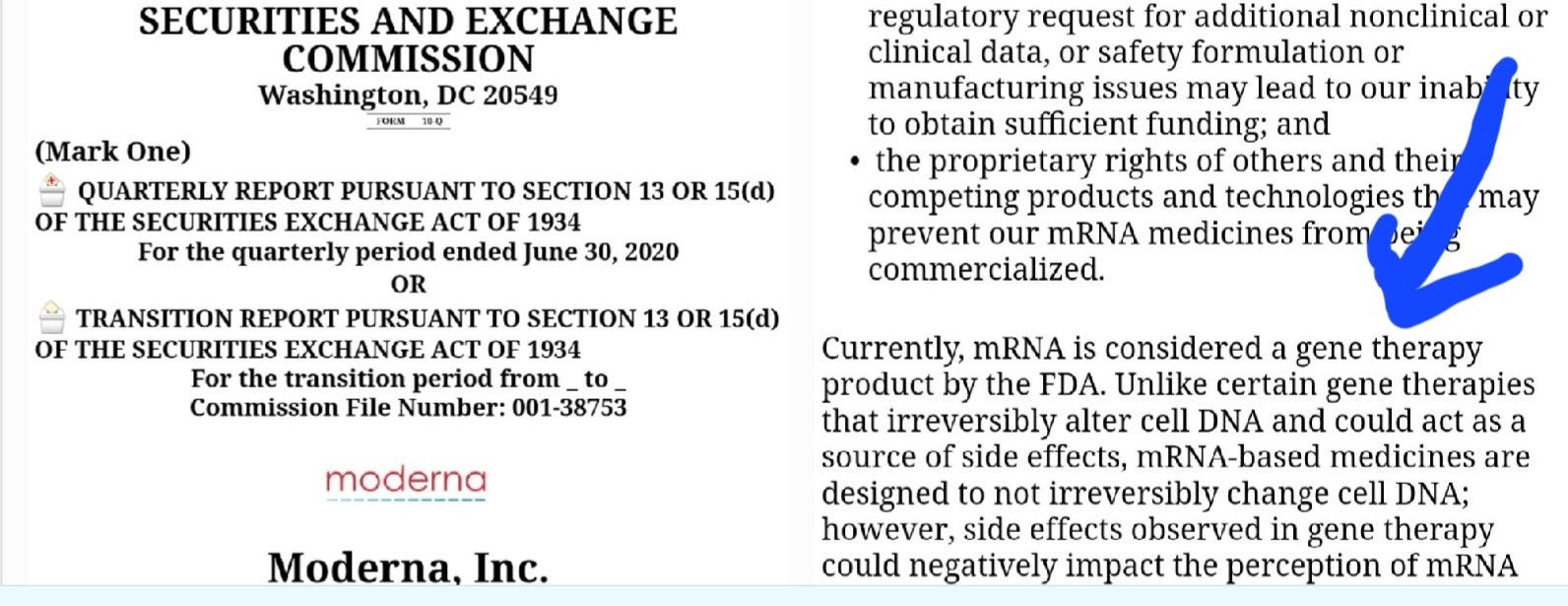
Moreover, one addition to this letter is to bring to your attention another crucial aspect of this issue that relates to the broader legal and ethical concerns around the Department of Defense’s mandates. It is critical to bring to your attention the ongoing legal and ethical issues surrounding the Department of Defense’s (DoD) mandate of experimental mRNA gene therapies for military personnel, which may also have serious implications for the veterans your department serves.
The Secretary of Defense (SECDEF) has bypassed legal protections outlined in 50 U.S.C. § 1520a (2021) by compelling service members to participate in a treatment that was not only experimental but also mandated without proper informed consent. This action directly contradicts federal law, which prohibits the mandatory use of experimental biological agents in military personnel. The products used in the mRNA gene therapy treatments, such as the COVID-19 vaccines and PCR testing, fall under the Emergency Use Authorization (EUA) category, which - by definition - requires voluntary participation. Under 21 USCS § 360bbb-3, it is unlawful to mandate these investigational products. As the SECDEF has issued a mandate for their use, it constitutes a direct violation of federal law that explicitly protects individuals' right to refuse participation in experimental treatments. The nature of these products as EUA treatments and not fully licensed vaccines under the FDA means that these products should never have been mandated, as per the guidance in 45 CFR 46.116, which emphasizes informed consent and voluntary participation.
The DoD’s actions have caused significant harm to service members who were subjected to these experimental treatments. Adverse reactions, including chronic inflammation, organ failure, and even tumors, have been reported. These injuries are linked to the unauthorized experimentation with biologics, a violation that can have long-lasting consequences for our veterans, many of whom may now be facing lifelong health struggles. The mRNA gene therapies, as ultrahazardous agents, pose a serious risk to the health of service members and veterans alike, and this harm can be traced directly to the DoD’s mandate.
It is also important to note that the SECDEF’s misrepresentation of these mRNA treatments as vaccines constitutes deceptive medical practices under 15 U.S.C. § 45(a), as the products do not meet the legal definition of vaccines and have not shown efficacy in preventing infection or transmission.
This is a matter of public trust, as veterans may have been misled about the nature and efficacy of the treatments they were required to take. In addition, the DoD's failure to adhere to its own ethical standards, as outlined in DoD 3216.02 and 45 CFR 46.116, raises further concerns regarding the treatment of military personnel and veterans in this regard.
Given the ongoing impact of these actions on the health of our veterans, I urge you to take this information into account as the VA reviews its protocols and Standard Operating Procedures (SOPs) in dealing with the aftermath of these mandated treatments. The potential for long-term health consequences for veterans affected by these experimental treatments is significant, and it is imperative that the VA takes steps to address the harm done by the SECDEF’s actions, ensuring that veterans are provided with the care and support they need.
• Bahl, K., et al. (2017). Preclinical and Clinical Demonstration of Immunogenicity by mRNA Vaccines against H10N8 and H7N9 Influenza Viruses. Molecular Therapy, 25(6), 1316-1327.
• Kowarz, E., et al. (2021). Vaccine-Induced Covid-19 Mimicry Syndrome: Splicing Errors of mRNA from BNT162b2/SpikeVax after Intramuscular Vaccination. Frontiers in Immunology, 12, 739833.
• Szebeni, J., et al. (2018). Complement activation-related pseudoallergy: a stress reaction in blood triggered by nanomedicines and biologicals. Molecular Immunology, 94, 122-132.
• Wang, Y., et al. (2022). DNA Contamination in mRNA Vaccines and Its Potential Health Risks. International Journal of Vaccine Therapy, 15(4), 203-215.
• National Defense Authorization Act (NDAA) for Fiscal Year 2006 - Section 705 (10 U.S.C. § 1107). This section of the NDAA restricts the use of "investigational new drugs" or biological agents in military settings unless specific criteria, including informed consent, are met, except in cases of very specific emergency scenarios.
• Emergency Use Authorization (EUA) (21 USCS § 360bbb-3). Under this statute, it is unlawful to mandate the use of investigational products that have been granted Emergency Use Authorization. It states that EUA products should only be administered voluntarily and not forced upon individuals.
• Federal Regulations for Informed Consent (45 CFR 46.116). This regulation governs the requirement for informed consent in the context of research involving human subjects. It emphasizes that participation must be voluntary and based on a full understanding of the risks involved.
• Department of Defense Directive (DoD 3216.02). This directive covers the ethical treatment of military personnel in research, including the requirement for voluntary participation and informed consent in any clinical research involving experimental treatments.
• Deceptive Practices in Advertising (15 U.S.C. § 45(a)). This section of the Federal Trade Commission Act prohibits deceptive practices in advertising, including misrepresentations about products. In this case, it refers to the misrepresentation of mRNA treatments as vaccines, as they do not meet the legal definition of a vaccine and have not shown the ability to prevent infection or transmission.
• Department of Veterans Affairs (VA) Informed Consent Regulations (38 CFR 16.116). This regulation ensures that veterans are fully informed and voluntarily consent to medical treatments and participation in clinical research. It emphasizes the need for clear communication regarding risks, benefits, and alternatives in treatment decisions.
• 21 U.S. Code § 360bbb-3 (Emergency Use Authorization): Pertains to the authorization for medical products to be used in emergencies under Title 21 of the U.S. Code, governing food and drugs. Specifically, it details conditions for Emergency Use Authorization (EUA) of drugs, biological products, and medical devices during public health emergencies.
• 21 U.S. Code § 360bbb-3(e)(1)(A)(ii)(III) requires that individuals receiving an EUA vaccine must be informed of their option to accept or refuse the vaccine, the consequences of refusal, and available alternatives.
• 15 U.S.C. § 45(a) (Deceptive Medical Practices): Under the Federal Trade Commission (FTC) Act, it is unlawful to advertise a product as capable of preventing, treating, or curing disease without competent scientific evidence substantiating the claims. This applies to the promotion of mRNA vaccines or other experimental products when such claims are made without proper clinical evidence.
• 7 CFR Part 731 (Biotechnology Regulations): Issued by the U.S. Department of Agriculture (USDA), this part governs the introduction of genetically engineered organisms into the environment, ensuring that such activities comply with safety protocols to protect human health and the environment.
• 9 CFR Part 121 (Select Agents and Toxins): Regulates the possession, use, and transfer of biological agents and toxins that pose a severe threat to public health and safety, animal health, or plant health. Violations could occur if gene therapy experiments involve select agents and fail to adhere to these strict regulations.
• 42 CFR Part 73 (Select Agents and Toxins): Similar to 9 CFR Part 121, this part specifically defines and regulates biological agents, including genetically engineered or synthesized agents, that are capable of causing severe harm, including death or disease, in humans, animals, or plants.
• 38 CFR 3.303 (Service Connection for Disabilities): This regulation outlines how the VA evaluates service-connected disabilities, including those related to toxic exposure, and could be applied to vaccine-induced injuries if recognized as part of Toxic Exposure Risk Activity (TERA).
• 38 CFR 17.38 (Medical Benefits Package for Veterans): This regulation describes the scope of care available under the VA’s health care system, potentially including vaccine-related injuries if acknowledged as part of VA health care benefits.
• 21 CFR 50.20-23 (Informed Consent in Human Research): These regulations require that informed consent must be voluntary and based on sufficient understanding of the research and its risks. Specifically, 21 CFR 50.23(d) allows the waiver of informed consent for military personnel under certain emergency circumstances. However, this waiver provision undermines the core principle of voluntary informed consent, especially in the context of military service members.
• 10 U.S.C. 1107(f) (Human Experimentation in the Armed Forces): This regulation governs the requirements for military personnel to participate in clinical trials or testing of investigational new drugs or biological agents. It mandates that informed consent must generally be obtained, except under limited circumstances where the President deems it infeasible.
Additional Scientific References: • Sahay, G., Aluri, S., & Racherla, S. (2020). Lipid nanoparticles for mRNA vaccine delivery: A review. Nature Biomedical Engineering, 4(12), 1065 1083. https://doi.org/10.1038/s41551-020-00637-7 • Allen, M., Chong, A., & Smith, R. (2021). Polyethylene glycol and its role in vaccine-induced immune responses. Vaccine, 39(1), 16-23. https://doi.org/10.1016/j.vaccine.2020.10.008 • Yoo, Y., Chen, M., & Lee, W. (2022). Inflammatory responses induced by lipid nanoparticles in vaccines: A review. Vaccine, 40(10), 1364-1376. https://doi.org/10.1016/j.vaccine.2022.01.004
Fantastic! It's been a long time coming that they acknowledge their abolishment of personal bodily integrity for military personnel. I will forward to our friend a General in the Army.






Fantastic! It's been a long time coming that they acknowledge their abolishment of personal bodily integrity for military personnel. I will forward to our friend a General in the Army.